Blog
Meet our Advisor: Ash Zenooz
Dr. Ash Zenooz is a unique figure in healthcare because she bridges the gap between three distinct worlds: the clinical (as a board-certified radiologist), the governmental (as former CMO for the VA’s EHR modernization), and the enterprise tech (as former CMO of Salesforce and CEO of Commure). At Commure, she had the vision of creating a universal platform. She often spoke with hospital execs about drowning in "pilot-itis"—hundreds of small tools that don’t talk to each other.
Advisor to actAVA.ai, Dr. Ash Zenooz has previously argued that the "era of point solutions is over." Our questions today move past "Will AI replace doctors?" and “What is the shift in thinking that is required to make it happen?” In brief, today we are focused on integration, scale, and the platform economy.
1. Moving from "Point Solutions" to a "Healthcare Operating System."
You’ve frequently stated that the era of 'point solutions' in healthcare is over. As AI becomes commoditized, how should health systems shift their strategy from buying individual AI tools to building a unified 'operating system' that actually scales across an entire enterprise?
The binary debate of platform versus point solutions is too clean. Point solutions are not going away in healthcare. If there's an FDA-cleared stroke-detection model or a specialized imaging algorithm integrated into a clinical workflow, health systems absolutely want the best tool for that specific job.
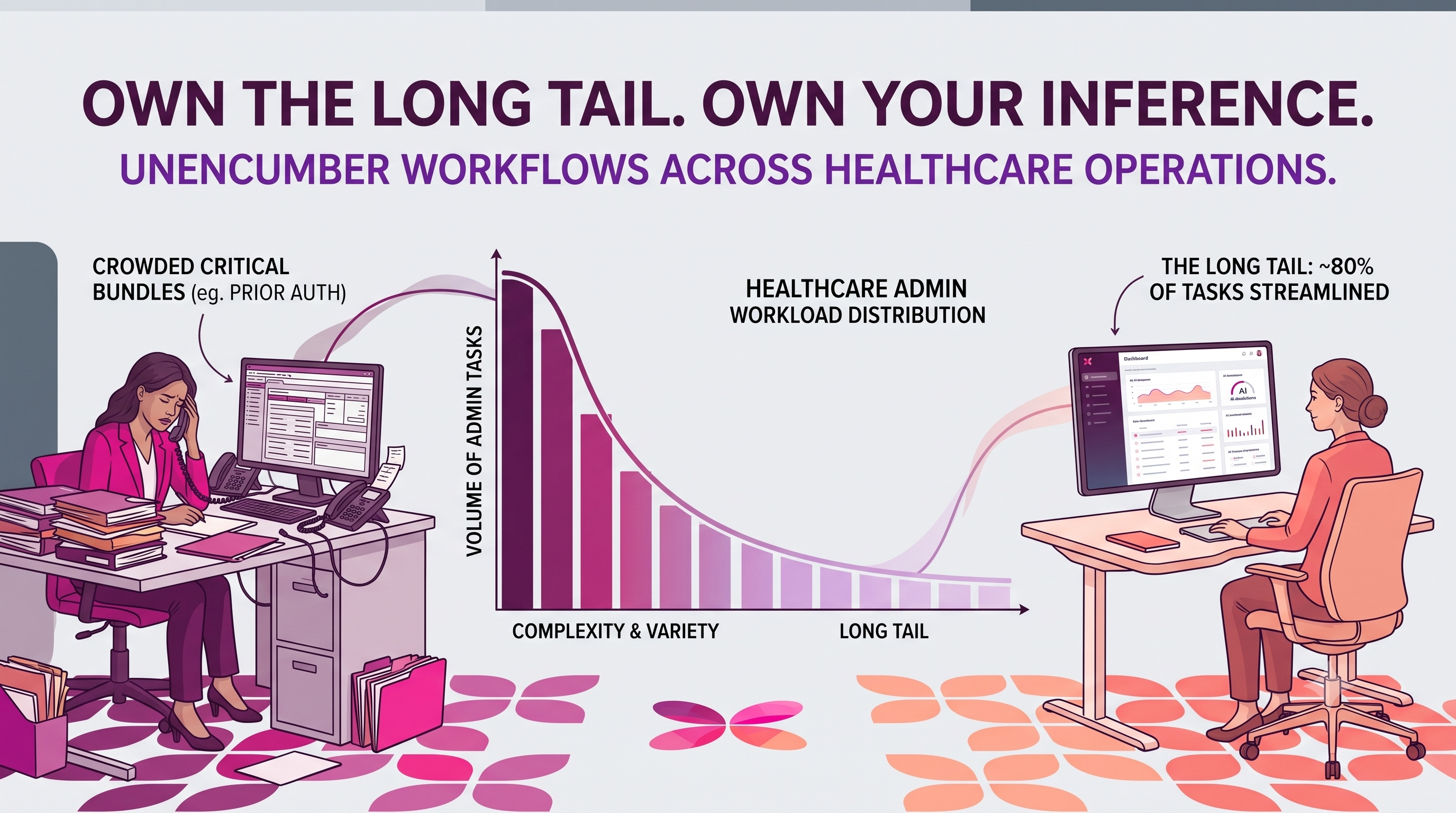
What broke the point-solution era was the explosion of disconnected tools. Health systems ended up with hundreds of products, each with its own workflow, login, governance process, and integration burden on IT teams.
But the answer isn't one giant vendor platform either. That just creates a different kind of lock-in. Once an AI strategy depends entirely on a single EHR vendor or AI company, the organization's roadmap becomes tied to that vendor's or company's priorities and release cycle.
What actually scales is an orchestration layer that sits above the core systems and connects workflows across the EHR, operations, and revenue cycle while allowing individual tools and vendors to change over time. Ultimately, the health systems that win will set up a structure to integrate, govern, and evolve AI without rebuilding the enterprise every few years.
2. Solving the "Invisible Work" and Clinician Burnout.
As a physician yourself, you are deeply attuned to burnout. There is a fear that AI efficiency will be used by administrators to squeeze more volume out of doctors. This question touches on the 'applied AI" aspect of your career and the ethical implementation of tech in a clinical setting. Beyond just saving time, how do we ensure that AI-driven efficiency actually returns humanity to medicine rather than just raising the quota for how many patients a doctor can see in an hour?
Healthcare is one of the few industries where costs keep rising despite all our technology. AI will clearly create efficiency, but the real question is what we do with that productivity gain.
There are three paths, and all of them look good on a spreadsheet. First, you can use AI to see more patients in the same amount of time. That's the historical default, and it's also the path to more burnout. Second, you can expand access to underserved populations, such as rural communities and behavioral health patients, who currently lack access to care. Third, you can give clinicians and patients time back so they can rebuild a relationship, which improves retention, quality, and long-term outcomes.
Ensuring the right path comes down to contract design and measurement. Payment models need to reward outcomes, not just volume. That means capitation or shared savings arrangements in which efficiency gains improve care quality and reduce friction, rather than simply increasing throughput. It also means measuring patient retention and quality scores, not just visit volume.
Without deliberate choices embedded in contracts and incentives, the system will default to volume. We've seen this before with EHRs.
3. The "Interoperability Paradox" and AI Readiness
You’ve managed some of the largest data modernization projects in history at the VA and Salesforce. We are now seeing a 'race for AI agents' in healthcare, but these agents are only as good as the data they can access. What is the biggest 'hidden' hurdle currently preventing healthcare data from being truly AI-ready at a global scale?
A decade ago, the problem was that systems couldn't connect. Today, with FHIR, APIs, cloud infrastructure, and TEFCA-like frameworks, we can move data. The harder problem now is whether the data means the same thing everywhere, whether it's complete, and whether an AI agent can safely act on it.
Healthcare data remains deeply fragmented, unstructured, and context-poor. The majority of clinically meaningful information lives in physician notes, PDFs, images, and faxes, which are not in clean, structured fields. Even within structured data, different organizations document the same clinical information differently. That creates a massive challenge for the safe deployment of AI at scale. When underlying data is incomplete or inconsistent, it becomes difficult to validate AI recommendations, audit decision-making pathways, or manage liability with confidence.
The irony is that the future advantage in healthcare AI may belong less to the one with the smartest model and more to whoever can create trusted, longitudinal, context-rich data environments that agents can work with safely.
Bonus Round
Since you are a radiologist, one of the first specialties to be "disrupted" by AI, here is a "lightning round" question: "As a radiologist, what is one thing AI has taught you about the limitations of human perception?"
AI has reinforced the extent of human perception's inconsistency. Two radiologists can look at the same scan at different times of the day and notice different things. Fatigue, cognitive bias, and context affect us more than we care to admit. AI, however, doesn't get tired on the 80th scan of the day. That's made me appreciate how human judgment and machine consistency complement each other.
More About our Advisor
Dr. Ash Zenooz leverages her medical background and enterprise technology expertise to build scalable, patient-centric solutions that bridge the gap between clinical needs and digital capabilities. She served as the Chief Executive Officer of Commure, a prominent platform company with a core mission to accelerate the development and deployment of next-generation healthcare applications. In this role, she steered the company toward building a secure, interoperable foundation essential for innovation across the healthcare ecosystem.
Prior to her tenure at Commure, Dr. Zenooz held a pivotal role at Salesforce, serving as its Chief Medical Officer. During her time there, she was instrumental in scaling the product's substantial growth and driving critical innovation in cloud-based healthcare solutions. Her leadership was crucial in demonstrating how a robust, cloud-based platform could revolutionize patient relationship management, care coordination, and provider engagement.
Her entire professional journey is characterized by a deep and unwavering commitment to transforming the healthcare industry. By leveraging her foundational medical background and extensive experience in enterprise cloud computing, Dr. Zenooz consistently creates impactful, scalable, and truly patient-centric solutions. Her focus remains on bridging the gap between clinical needs and technological capabilities to enhance global care delivery and outcomes.