Blog
Own Your Long Tail Workflows, Own (some of) Your Inference
Every AI vendor is crowding into prior authorization, and CMS-0057 is turning it into a commodity feature. Meanwhile 80% of healthcare's administrative work sits untouched, because each of those workflows is too small for anyone to build a company around. That's your long tail, spanning care management, appeals and grievances, enrollment reconciliation, revenue cycle, and provider operations, and it's where your margin leaks and your staff burn out. This piece breaks down why no point solution will ever build for it, why the token economics (a $15 to $25 labor task runs for $1 to $2 in inference) reward whoever owns the workflow and the model calls behind it, and why owning your long tail beats renting yet more point tools.
By Kevin Riley
Own Your Long Tail Workflows, Own (some of) Your Inference
A hundred vendors are fighting over one workflow. While they crowd into cramped workspaces like “prior authorization”, roughly 80% of healthcare's administrative work sits untouched. That 80% is your burden, but it is also your opportunity to own it.
Keeping with our prior auth example, this very important workflow has become the most crowded corner of healthcare AI, and the CMS-0057 rule is turning it into a commodity feature every vendor will ship. That's fine. It also means the real opportunity lies elsewhere.
Your long tail is where your margin leaks, your staff burns out, and no point solution software company is coming to help. Here's why that gap exists, and why the smart move is to own these workflows and the inference that runs them.
The long tail dwarfs the fight over “prior auth”
The medical industry spends about $83 billion a year on staff time for 9 routine administrative transactions between providers and health plans. Prior auth is 1 of those 9. Eligibility, claims, remittances, enrollment, care management, medical policy management, appeals and grievances, network administration, and the rest make up the other 8, and hundreds of smaller workflows branch off from there.
Add it up and the long tail accounts for a large share of the roughly $500 billion healthcare spends every year on billing and insurance-related administration. Most of it still runs on people, phones, faxes, and portals.
Why no vendor builds for it
Point solutions need each workflow to be a big enough market on its own. Point solutions can raise money to automate prior auth because millions of cases run through it daily. They won't raise the funds to help you upgrade your current Care Management with the agents you need. Neither will they focus on automating 834 enrollment reconciliation, draft appeal letters for a mid-size plan, or validate provider directories under the No Surprises Act.
Each of those is real work and real cost. Each one is too small to build a company around. So they stay manual, not because they're hard to automate, but because the software math never lines up. The long tail is underserved by design.
A few workflows hiding in the tail
- Care management, from cohorting to planning to outreach to care follow up.
- Appeals and grievances, from intake triage and case assembly to deadline tracking and resolution letters.
- Enrollment reconciliation, including 834 discrepancies and Medicaid redetermination outreach.
- Revenue cycle beyond PA, like denial management, appeal letters, underpayment identification, and coding backlog triage.
- Provider operations, covering credentialing, directory validation, and roster reconciliation.
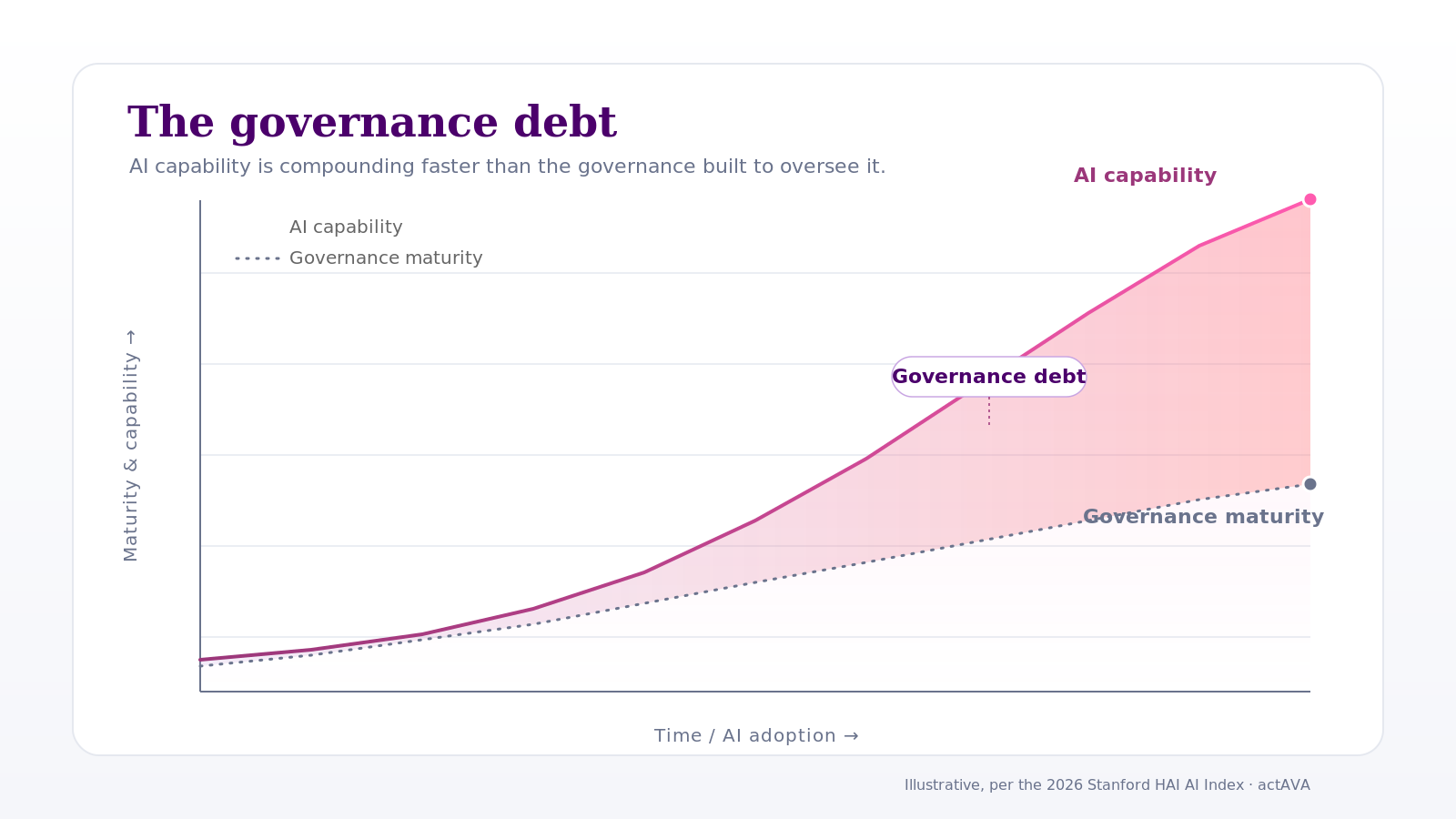
The economics that decide who wins
Here's the part that reshapes the whole decision. A knowledge task that costs $15 to $25 in labor converts to roughly $1 to $2 in tokens once an agent runs it. Call it a 10-to-1 ratio.
That gap is the prize, and it goes to whoever owns two things: the workflow and the inference underneath it. Rent a per-seat tool, and the vendor keeps the spread. Own the workflow and the model calls behind it, and the savings, the control, and the data stay with you.
The teams that win the next decade of healthcare operations will treat the other 80% as theirs to own.
Why owning it beats renting it
Your long tail is specific to you. Your plans, your policies, your systems, your edge cases. A generic tool built for the average customer will never fit the parts of your operation that actually differ, and the long tail is exactly where that difference lives.
Own the build, and you shape the roadmap instead of waiting on someone else's. Own the inference, set cost per task, keep sensitive data within your walls, and compound gains as your agents learn how your team actually works. Every workflow you bring in-house makes the next one cheaper to add.
Rent it, and you get the reverse. Someone else's priorities, someone else's margin, your data on their servers, and a bill that climbs with every seat you add.
Where this leaves you
The vendors piling into prior auth are competing for one square of a very large board. The long tail is wide open, and it's defensible in a way a single crowded workflow never will be, because owning it means owning your operating infrastructure rather than a feature.
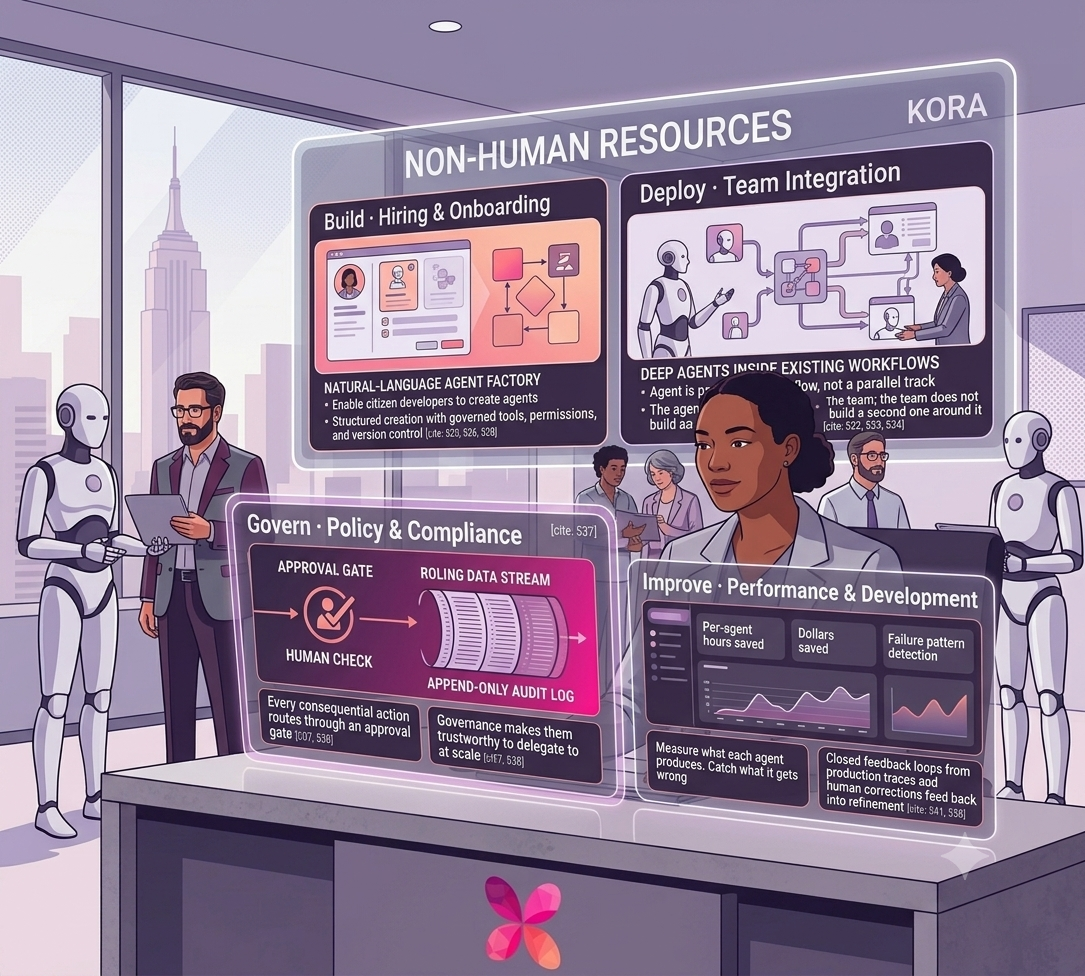
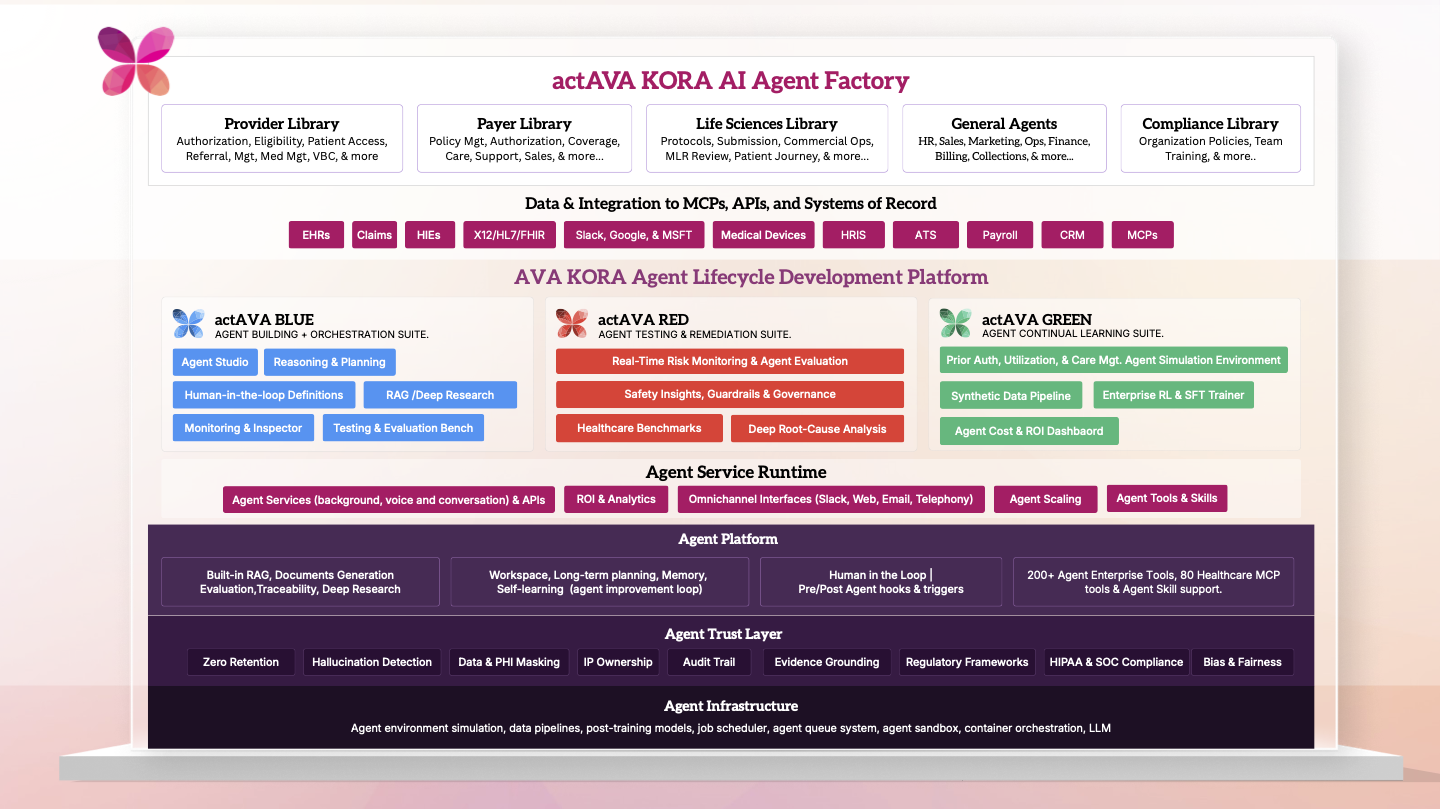
That's the case for building on a platform instead of buying yet more point solutions. At actAVA, we build the factory that lets healthcare organizations design, govern, and run their own agents across the long tail, with the inference under their control. Engineered chaos in, governed intelligence out, at the scale the work actually demands.
Want to see what owning your long tail looks like in practice?
Explore the workflows at actava.ai
Written by
Kevin Riley
CEO & Co-Founder