Blog
Why Healthcare Needs a Specialized RAG
Generic AI retrieval systems often fail in healthcare because they lack the robust infrastructure required to maintain patient context, ensure clinical accuracy, and enforce strict HIPAA compliance. To solve this, actAVA developed AVA, a specialized RAG architecture that utilizes advanced memory structures, verifiable citations, and multi-hop reasoning to safely support complex clinical decisions.
By Weiran Yao
At actAVA, we are often asked why we didn’t just wrap a standard LLM in a generic retrieval system and call it a day. The answer lies in the specific, high-stakes nature of medicine.
In the general tech world, Retrieval-Augmented Generation (RAG) is the gold standard for fixing AI hallucinations. It fetches data and feeds it to the model. But in healthcare, a generic RAG is like a brilliant medical student who has read every textbook but has no memory of the patient they saw ten minutes ago, and no understanding of hospital protocol.
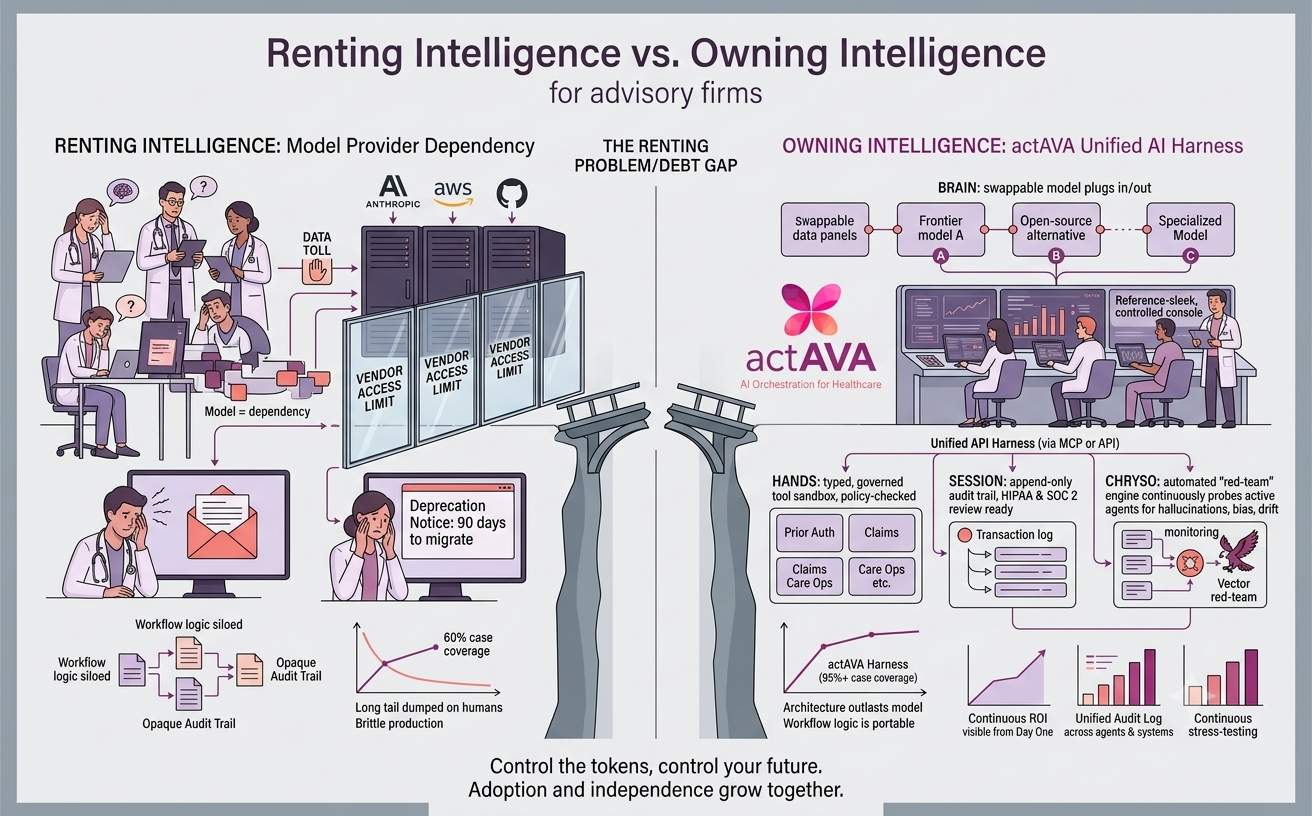
Healthcare AI adoption fails not because models lack capability, but because production systems lack the infrastructure to maintain context, ensure accuracy, and enforce compliance. That is why we built AVA, our specialized RAG engine designed specifically for the life sciences, as a foundation to our KORA agent-building platform.
1. The "Goldfish Memory" Problem
Generic RAG implementations retrieve information well, but they are terrible at maintaining conversations. Standard context windows fill up quickly. In a complex clinical consultation, critical details from the start of the session are often "truncated" (forgotten) by the time the doctor reaches the diagnosis.
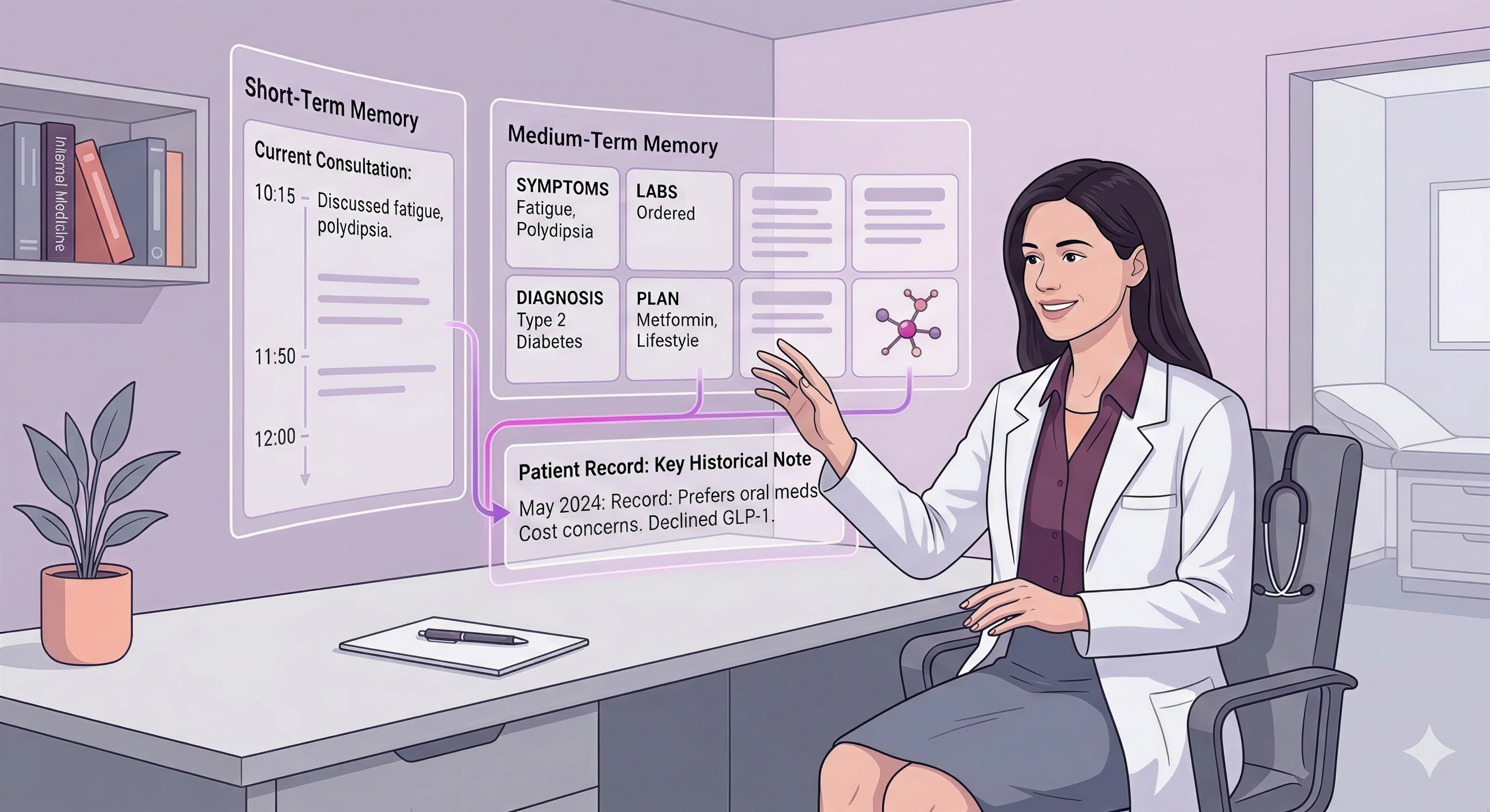
To solve this, we couldn’t rely on a flat memory structure. We built a Three-Layer Memory Architecture that mimics how a clinician thinks:
Short-Term Memory (Session Context): Handles the immediate "working memory" of the current consultation.
Medium-Term Memory (Structured Compression): This is our "secret sauce." When a session gets long, we don't just delete old text. AVA uses an intelligent 8-section compression technique to summarize key findings, decisions, and unaddressed concerns, keeping the context alive without blowing the token limit.
Long-Term Memory (The Patient Record): Persistent storage of history, preferences, and care plans that survive across different sessions.
This ensures that if a patient returns three months later, AVA doesn't just know "diabetes guidelines"—it remembers this patient declined a GLP-1 agonist last time due to cost.
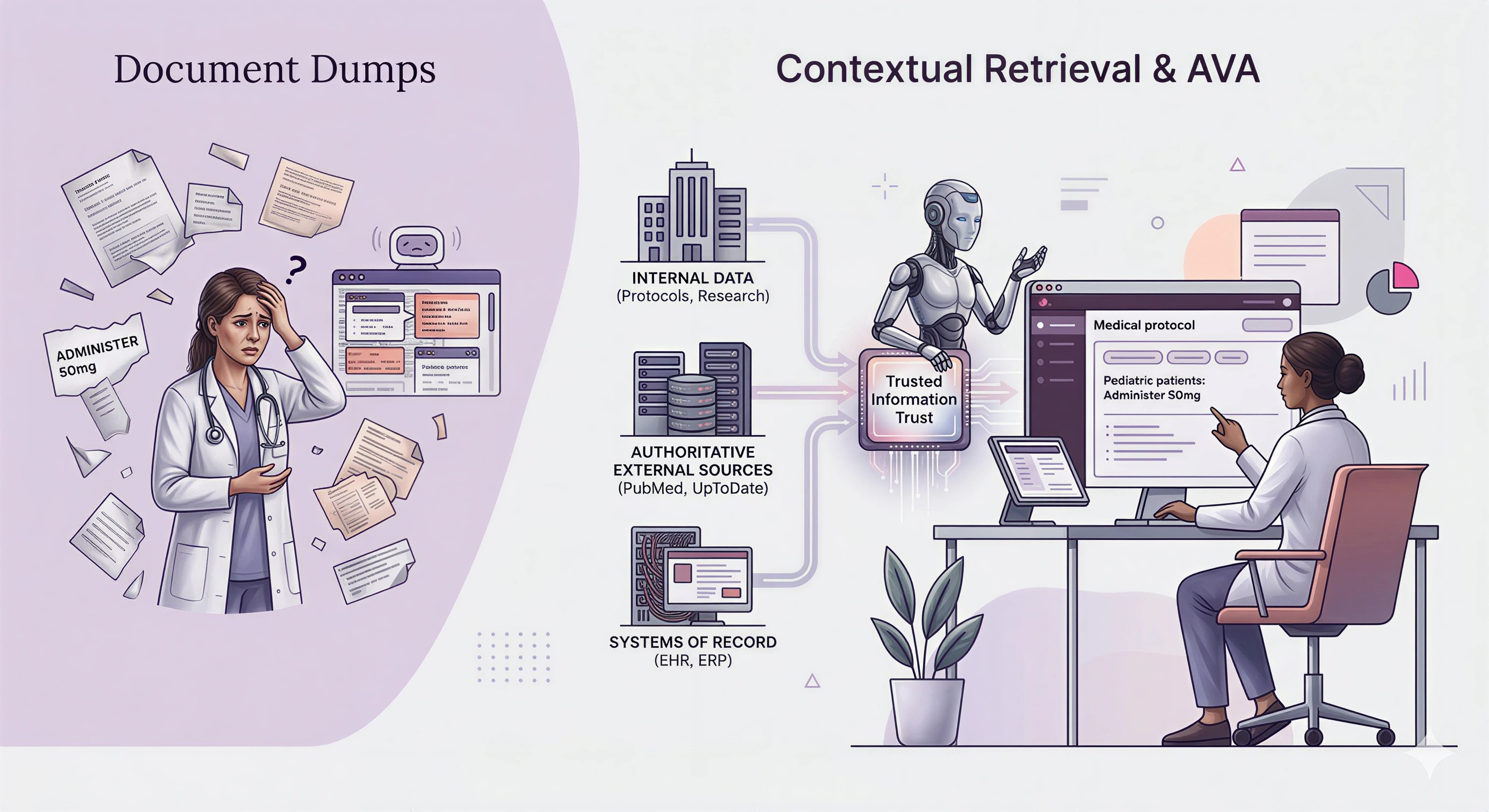
2. Contextual Retrieval vs. "Document Dumps"
Standard RAG systems chop documents into small chunks. The problem? When you chop a medical protocol into isolated paragraphs, you lose the surrounding context. A chunk might say "Administer 50mg," but without the previous paragraph, you don't know it applies only to pediatric patients.
We utilize Contextual Retrieval. We don't just index text; we index the meaning and metadata surrounding it. Furthermore, AVA is not a "closed box." While we support private, air-gapped corpora, healthcare requires a Hybrid Retrieval Architecture.
AVA retrieves from:
Your Internal Data: Protocols, policy docs, and proprietary research.
Authoritative External Sources: Live access to PubMed, UpToDate, and drug databases.
Your Systems of Record: Such as your ERP, EHR, or CRM.
This prevents the "silo" problem. A purely closed system is dangerous because it fails to incorporate updated contraindications. A purely open system is noisy. KORA blends both to create a "Trusted Information Trust."
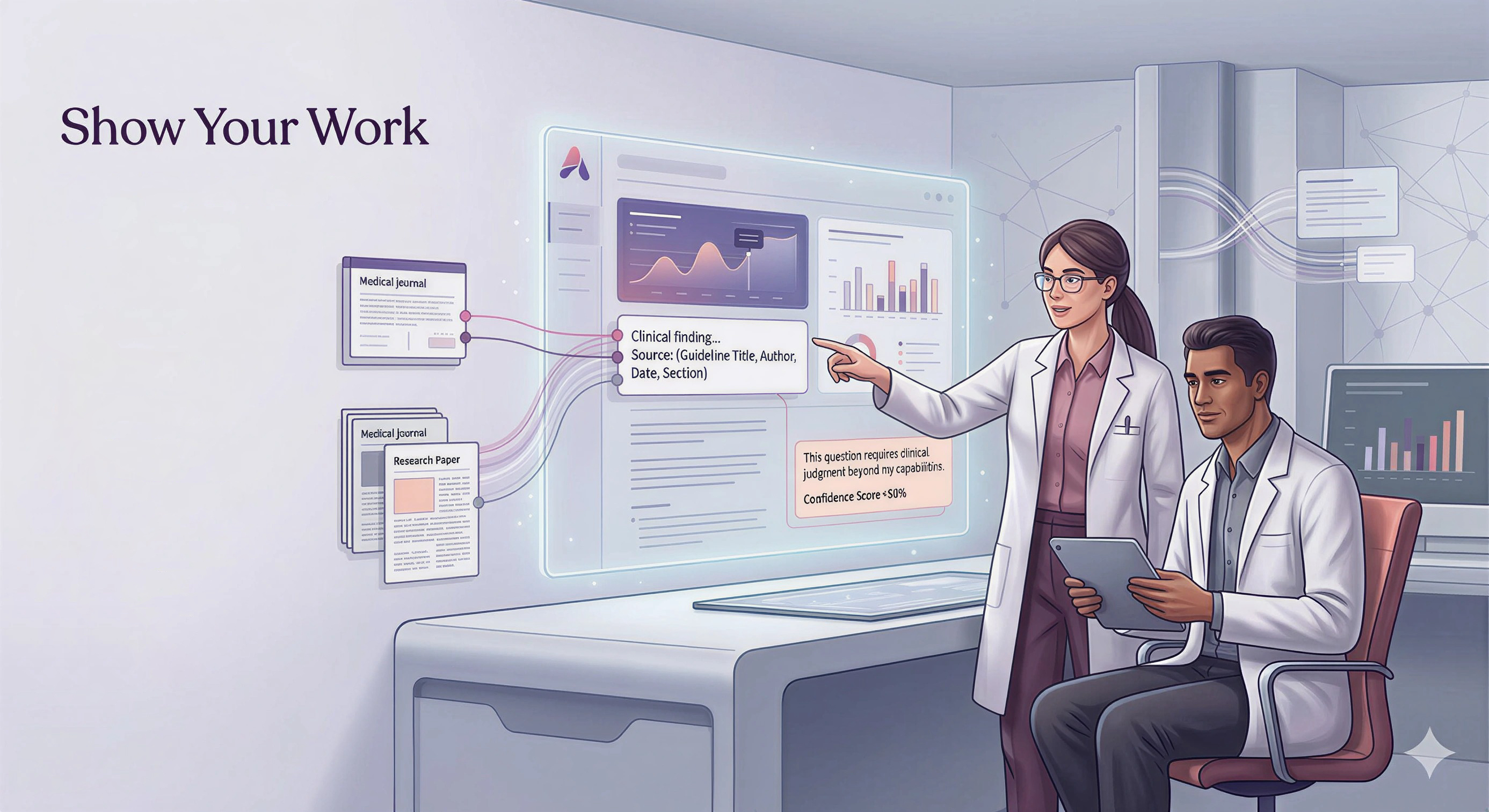
3. "Show Your Work": Auditability & Citations
In creative writing, a hallucination is imagination. In healthcare, it’s a malpractice suit.
A specialized healthcare RAG cannot simply give an answer; it must provide the evidence chain. We built AVA to be architecturally honest.
Citation-Backed Insights: Every clinical claim AVA generates is tagged with source metadata (Title, Author, Date, Section).
Traceability: Users can click through to the exact guideline or paper that drove the decision.
Abstention: If the confidence score drops below a specific threshold (e.g., <50%), AVA is programmed to explicitly state: "This question requires clinical judgment beyond my capabilities."
We don't just want the AI to be right; we want it to be verifiable.
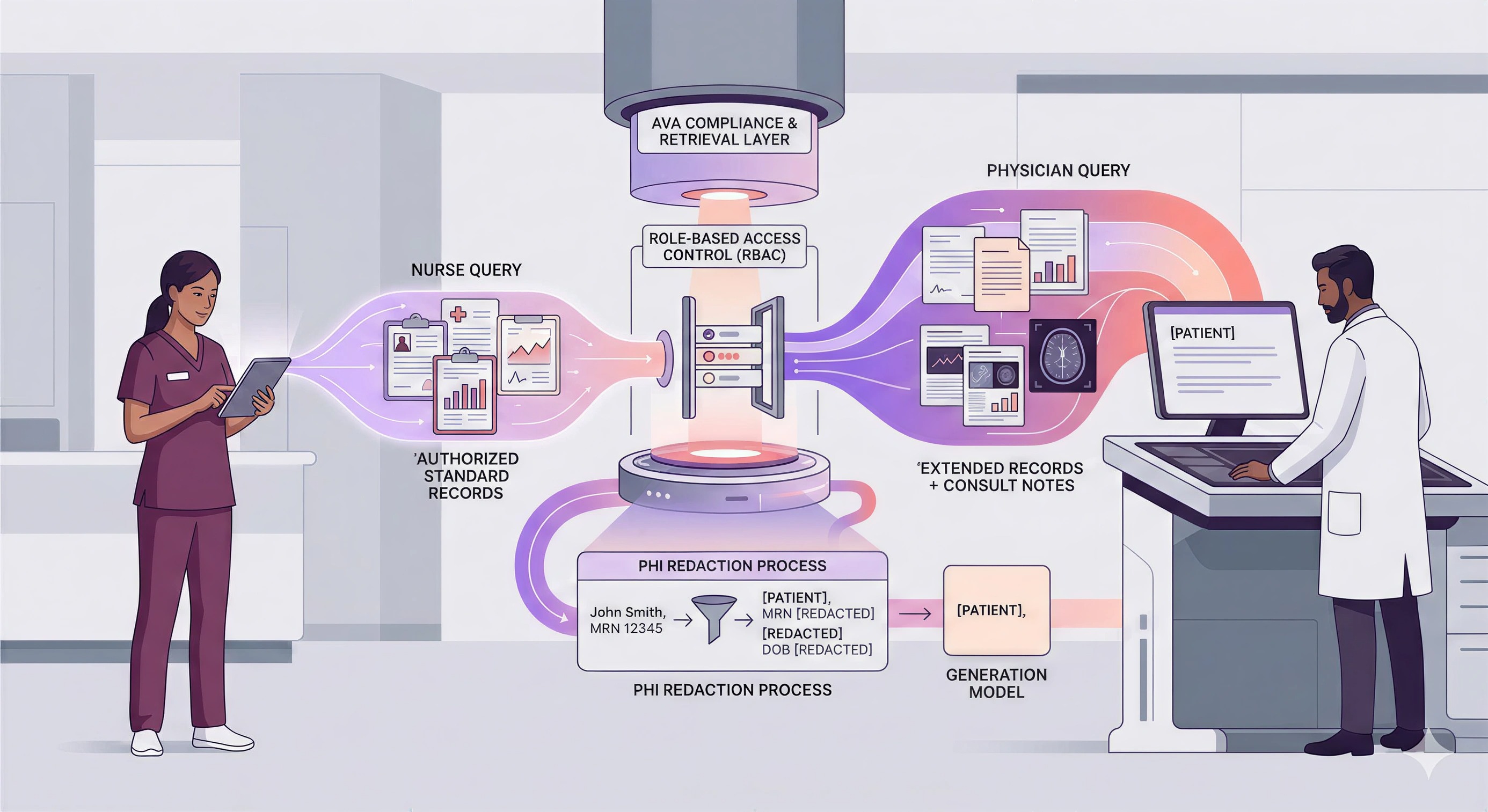
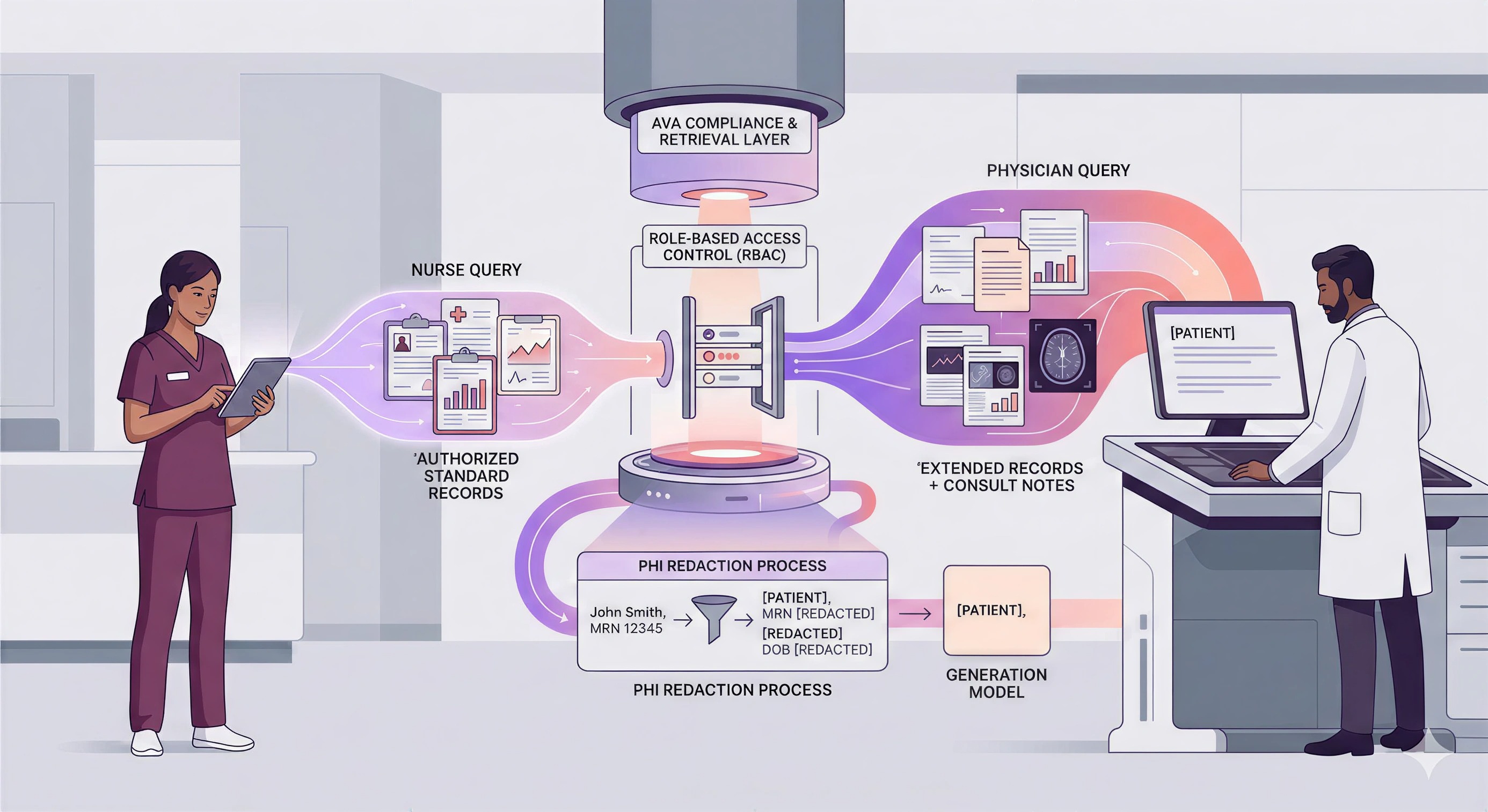
4. HIPAA is Not a Feature, It’s the Foundation
You cannot bolt compliance onto a general-purpose AI agent after the fact. It has to be baked into the retrieval layer.
AVA enforces Role-Based Access Control (RBAC) at the retrieval level. If a nurse asks a question, RAG retrieves only the documents the nurse is authorized to see. If a physician asks, the scope expands.
Furthermore, we handle PHI (Protected Health Information) with extreme care. Before any data is sent to a generation model, our system performs real-time redaction/anonymization. The AI reasons on "[PATIENT]," not "John Smith, MRN 12345."
5. The Deep Research Difference
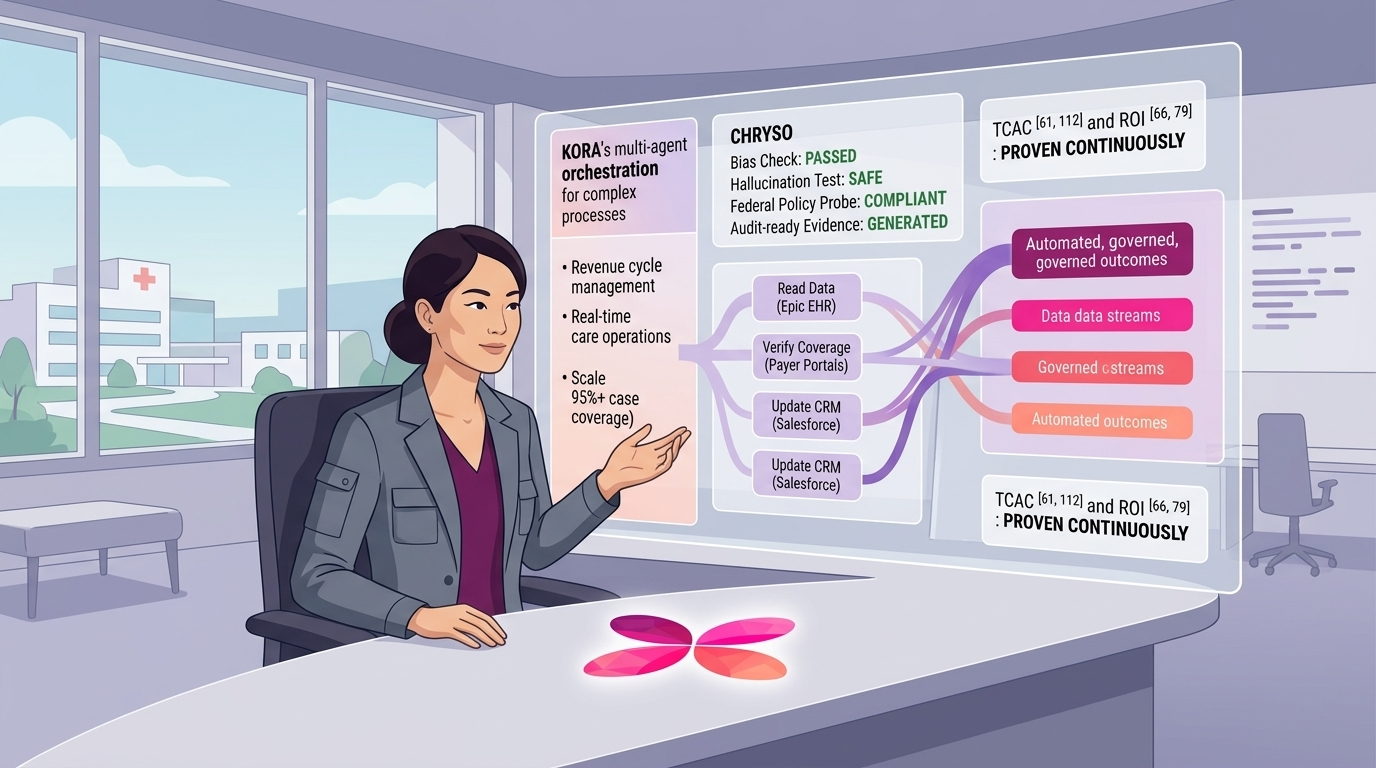
Finally, healthcare isn't just about Q&A; it's about synthesis. A specialized RAG needs to be an agent, not a search bar. AVA’s Deep Research capabilities allow it to perform multi-hop reasoning. It can:
Read a patient’s latest lab results (EHR).
Identify a decline in kidney function.
Cross-reference this with the patient's current medication list.
Retrieve the latest ADA guidelines on renal dosing.
Suggest a specific dose adjustment with citations.
This is the difference between a chatbot and a clinical infrastructure.
In conclusion, we think that healthcare doesn't need another wrapper for GPT-4. It needs an infrastructure that remembers like a clinician, researches like a medical librarian, and complies like a HIPAA officer. Our KORA platform takes this into account and solves the problem with our specialized RAG, AVA.

Written by
Weiran Yao
CAIO & Co-Founder